Fractured Maxillary Tuberosity
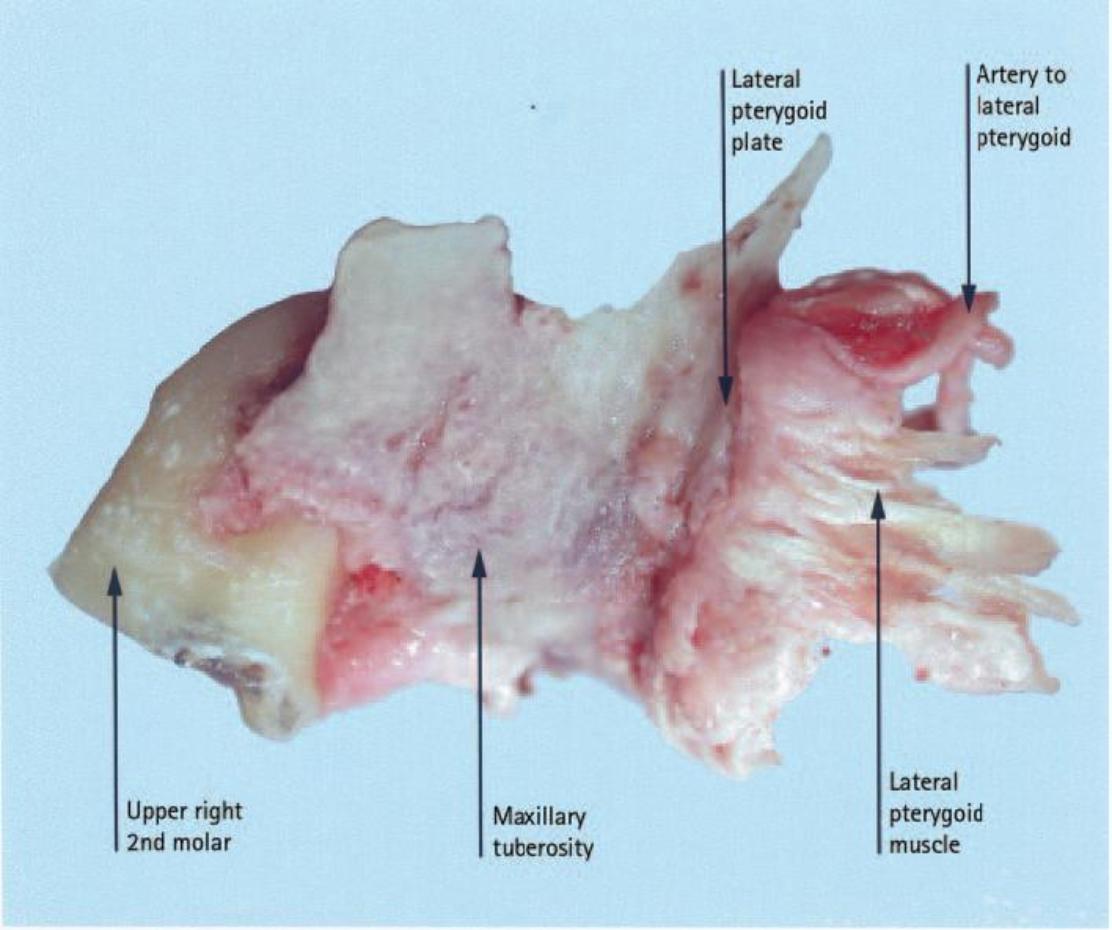
The maxillary tuberosity is the most hind-most (distal) aspect of the upper jaw (maxilla), housing the sockets of the upper wisdom teeth, with its back (posterior) border curving upward and distally.
The upper wisdom tooth lies just in front and within the maxillary tuberosity.
When an upper premolar / bicuspid (rare) or an upper molar (more likely) is extracted, there is a risk that the bony socket comes out with the tooth. This is mainly the roof of the mouth side). This is often accompanied by tearing of the gum (both cheek and roof of the mouth side, but mainly the roof of the mouth side).
The fracture of a large portion of bone in the maxillary tuberosity area is a situation of special concern. The maxillary tuberosity is especially important for the stability / retention of upper dentures and may cause a mouth-sinus comminication (oro-antral communication).
If there is a large maxillary tuberosity fracture, the aim is to salvage the fractured bone in place and to provide the best possible environment for healing.
Routine treatment of the large maxillary tuberosity fractures is to stabilise the mobile part(s) of bone with rigid fixation techniques (i.e. splinting with archbars or immobilisation with a plastic splint) for 4 – 6 weeks.
Following adequate healing, a surgical extraction procedure may be attempted. However, if the tooth is infected / symptomatic at the time of the tuberosity fracture, the extraction should be continued by loosening the cuff of gum and removing as little bone as possible while attempting to avoid separation of the tuberosity from the layer of skin immediately overlying the bone (periosteum).
If the attempt to remove the attached bone is unsuccessful and the infected tooth is delivered with the attached tuberosity, the tissues should be closed with watertight stitches (sutures) as there may not be a clinical oro antral communication.
The Oral Surgeon may elect to graft the area after 4 – 6 weeks of healing and post-operative antibiotic therapy. If the tooth is symptomatic but there is no frank sign of purulence or infection, the Oral Surgeon may elect to attempt to use the attached bone as an autogenous graft.


The factors predisposing to a fractured maxillary tuberosity during extraction of upper molars are:
Tooth-Related Factors:
- Bulbous roots
- Dilacerated / divergent roots
- Fused roots
- Multi-rooted
- Lone-standing / last standing molars
- Deeply Impacted Maxillary 3rd Molars
- Hypercementosis
- Ankylosis
Surrounding Anatomy:
- Large sinus, expanding to extent of tuberosity
- Roots into sinus
- Resorbed maxilla (especially following premature loss of the 1st molar)
- Sclerotic tuberosity
Pathological Factors:
- Large peri-apical infection
- Cystic change
Procedure-Related Factors:
- Unsupported extraction technique
- Removal of multiple maxillary teeth leaving the most distal one to the last
- Excessive force is used to remove the tooth
Not only forceps extraction of a resistant second or third molar but also first molar may result in fracture of the maxillary tuberosity.
All Oral Surgeons who practice exodontia must be able to manage this complication, immediately the problem occurs.